
Hip Arthroscopy, Sports Hip Injuries and FAI



Hip surgery has advanced immensely in the last twenty years and it is no longer confined to hip replacement surgery in older patients with osteoarthritis or fractures. Hip problems can affect adults of all ages. Better hip replacement implants and surgical techniques have made hip replacement surgery applicable to a much wider age group to allow return to normal activity. In addition, the advent of advanced MRI and CT scanning and direct visualisation of the hip with arthroscopy has lead to a much greater understanding of hip pain that is not caused by arthritis. Sporting hip injuries can be identified and treated, as well as shape abnormalities of the hip that can predispose to arthritis in young adult life. Fortunately, if recognised early enough, these shape abnormalities can be corrected to delay or even prevent arthritis developing all together.
Whilst arthroscopic (keyhole) surgery to large joints such as the knee and the shoulder is widely used, arthroscopy of the hip is performed much less frequently. The aims of surgery include repairing the damaged labrum with suture anchors, stabilising the cartilage and reshaping the femoral head so that it is spherical. Fortunately, modern equipment and advances in surgical technique have made arthroscopic hip surgery safe and reliable surgery in the hands of experienced surgeons. Mr Bankes has been performing hip arthroscopy since 2003 and has performed over 2,000 arthroscopic hip operations.
The key feature to understanding sporting hip injuries is that the pain comes from damage to structures at the front of the hip joint, namely the acetabular labrum and the articular cartilage at the front edge of the hip joint. It is for this reason that the symptoms are similar, irrespective of the type of injury, ie whether the labrum is torn, the cartilage is detached or a combination of the two. In addition, the symptoms are similar regardless of the cause of hip injury be it FAI, hip dysplasia or a simple labral tear without predisposing bony abnormality. Activities associated with hip injuries include running, rugby, martial arts, squash, tennis, hockey, football and dance.
Symptoms of hip injury
X-rays and scans
Femoroacetabular Impingement (FAI)
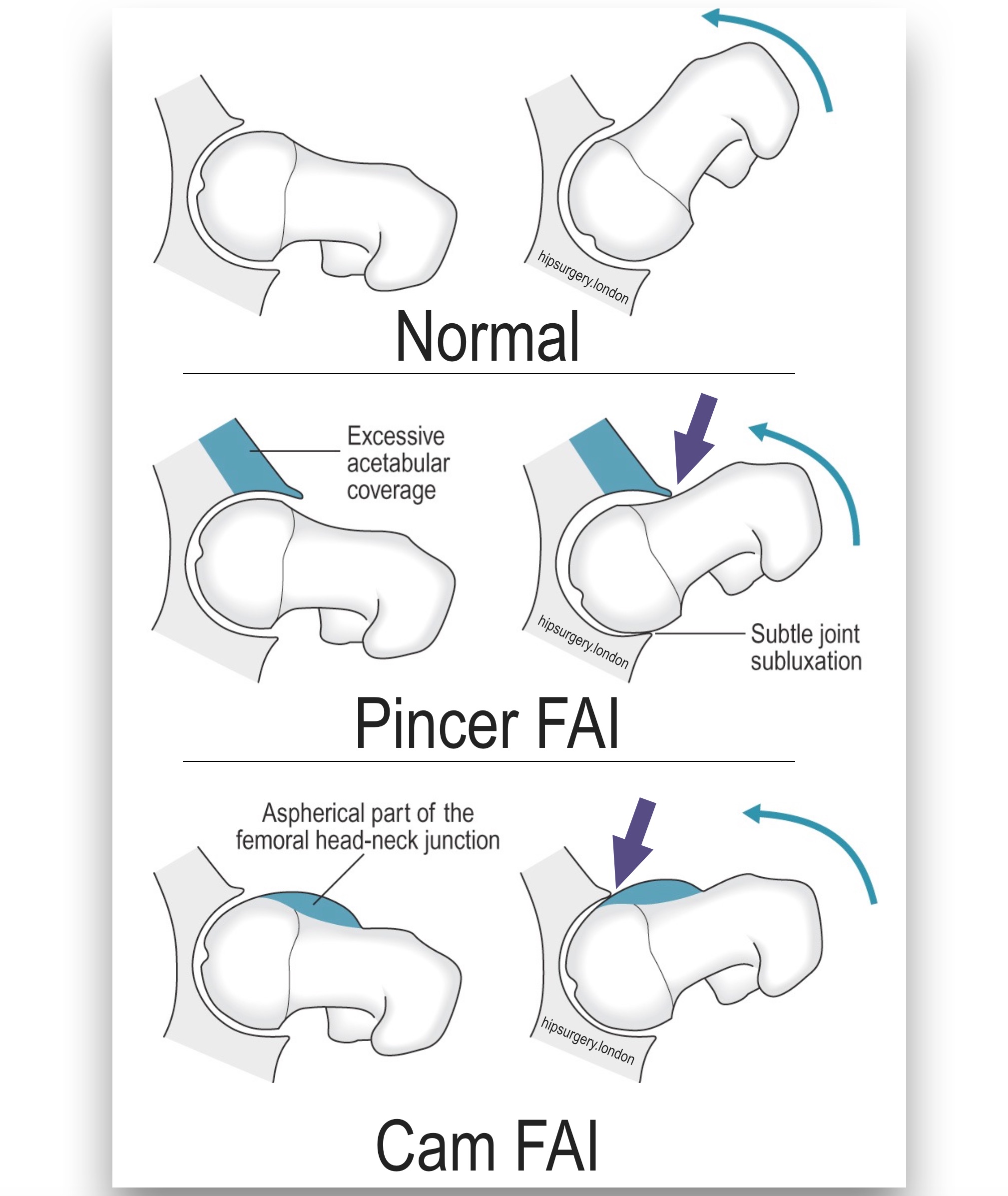 Femoroacetabular impingement (FAI) is a cause of tears to the acetabular labrum and damage to the front rim of the hip socket that may, over many decades, lead to osteoarthritis of the hip. In a normal hip, the ball of the ball and socket joint is perfectly spherical and sits inside a spherical socket so that there are no mechanical conflicts with movement in any direction. Hip joints in FAI, however, are not perfectly shaped: impingement hips have a flattening (the cam or the “bump”) at the front of the ball, which catches on the labrum and cartilage at the front of the socket with flexion and rotation movements, eventually causing damage. The cam itself develops as part of skeletal growth during childhood and adolescence but does not cause any symptoms until it has caused damage to the labrum and socket. Damage is cumulative and depends on the size of the cam, the ability of the labrum and cartilage to withstand injury, and the duration and intensity of activity. Age of onset of symptoms is typically in the 30s and 40s, although it is increasingly common to see symptoms in teenagers.
Femoroacetabular impingement (FAI) is a cause of tears to the acetabular labrum and damage to the front rim of the hip socket that may, over many decades, lead to osteoarthritis of the hip. In a normal hip, the ball of the ball and socket joint is perfectly spherical and sits inside a spherical socket so that there are no mechanical conflicts with movement in any direction. Hip joints in FAI, however, are not perfectly shaped: impingement hips have a flattening (the cam or the “bump”) at the front of the ball, which catches on the labrum and cartilage at the front of the socket with flexion and rotation movements, eventually causing damage. The cam itself develops as part of skeletal growth during childhood and adolescence but does not cause any symptoms until it has caused damage to the labrum and socket. Damage is cumulative and depends on the size of the cam, the ability of the labrum and cartilage to withstand injury, and the duration and intensity of activity. Age of onset of symptoms is typically in the 30s and 40s, although it is increasingly common to see symptoms in teenagers.Whilst early symptoms of FAI can be treated with physiotherapy and activity modification, surgery is the only way of removing the cam and correcting the mechanical abnormality. The aims of surgery include tidying up the damaged labrum and cartilage and reshaping the femoral head so that it is spherical. Any additional prominence of the socket at the front can also be dealt with at the same time. The aim of surgery is to relieve pain and restore movement, but clearly it also improves the mechanics of the hip so that progression of damage is stopped or slowed. It also follows that surgery is most effective before the damage to the hip is too severe. Surgery for FAI has evolved rapidly over the last decade and the type of surgery depends on the location and types of bony abnormality and the patient’s age. Whilst the majority of FAI can be treated arthroscopically, it is also important to appreciate that some deformities can only be comprehensively treated with open surgery. Undertreatment may lead to persisting or recurrent symptoms and the inconvenience and unpredictability of repeat surgery. Surgery should be considered in symptomatic elite and professional athletes or when:
- Symptoms are starting to affect day-to-day activity or walking
- Exercise remains affected despite reducing intensity
- Symptoms have been present for at least 6 months and are deteriorating / not improving
- Non-surgical treatments have not been effective
Frequently asked questions
This is a hidden item please do not touch
Surgery is can be performed as a day case although often it is more convenient for patients to stay overnight if surgery finishes late afternoon or early evening. Patients are advised to use crutches for two weeks to allow the post-operative pain to subside and also to perform basic hip exercises taught by the physiotherapist prior to discharge from the hospital. It is normal to have bruising and swelling around the three small incisions, particularly the one at the front.
Patients are advised to take two weeks off work, but clearly, this varies between individuals, particularly as working from home in some capacity is possible for many. Patients should not do any work at all during the week of surgery and the week after so there are no distractions to recovery. Some work from home is reasonable in the second week, with a potential return to the office for the odd half-day. The hip feels comfortable for day-to-day activities after four to six weeks and a full recovery is really determined by patients’ sporting aspirations: clearly, it takes less time to recover sufficiently to play golf compared with competing in a triathlon. As a general guide running and team sports are possible after four to six months.
If patients are confident walking without crutches and able to enter a car unaided then a return to driving is reasonable after two weeks.
Physiotherapy is absolutely vital following surgery for FAI with 10-12 sessions being required over 4-5 months. Weekly physiotherapy sessions are started after a couple of weeks to regain hip movement and core and hip strength. Use of a static bike and pool is encouraged from two weeks postoperatively. Muscles take many weeks to recover not only from the surgery but also, more importantly, the long-term effect of the hip injury itself prior to surgery. After a couple of months, physiotherapy can become more spaced out as the emphasis on rehabilitation moves from the physiotherapy practice to the patient’s own gym. As the surgical discomfort subsides patients become more confident in achieving goals set by their physiotherapist, with a step-wise move up from static bike, to elliptical trainer after about six weeks and finally treadmill. Squats and deep lunges are not advised for at least 3 months after surgery because these activities cause unnecessary irritation to the area of bone removal. Patients are not encouraged to run for at least four months after surgery.
No. Stitches are dissolvable and the dressings can be removed after ten days.
Complications after keyhole hip surgery are unusual. Patients may experience temporary soreness or numbness in the foot from the traction boot applied to gain access to the hip joint during surgery. Temporary swelling, bruising and clicking around the hip area are also entirely normal after hip arthroscopy and resolve within two to three weeks. Temporary stretching injuries to the major nerves in the leg are very rare following hip arthroscopy. The most important complication is that the surgery may not succeed in its goals of relieving pain and improving activity levels. In published studies, 65 – 75% of patients are pleased with their surgery and would undergo the procedure again on the other hip if necessary. Even if surgery is not successful patients still notice, with time, that they are no longer deteriorating. Surgery is least likely to be successful when the cam has already done a lot of damage to the cartilage and the hip is on the verge of arthritis. These borderline hips can usually be identified with pre-operative x-rays and scans so patients can be warned. Arthroscopic surgery also has the advantage that it starts with a direct examination of the joint and occasionally, unexpectedly severe arthritis is found.
Patients are expected to have a supply of paracetamol and ibuprofen (Nurofen, the non-steroidal anti-inflammatory drug) at home. In addition, they are sent home with a few days’ supply of stronger painkillers such as codeine or tramadol.
Links
Introduction to Hip Impingement (FAI) Marcus Bankes speaks at the Fortius International Sports Injury Conference 2015 (FISIC).